
Venous Reflux Is Not a Diagnosis
An educational discussion, not medical advice
A recurring misunderstanding
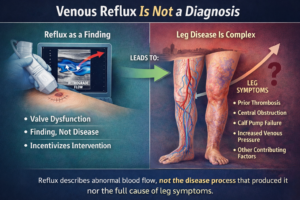
In discussions of vascular health, venous reflux is often spoken about as if it were a diagnosis in itself. A duplex ultrasound demonstrates reflux, the finding is labeled, and it can quickly become the focal point of interpretation and next steps. The unspoken assumption is straightforward: reflux explains the symptoms, and addressing reflux will resolve the problem.
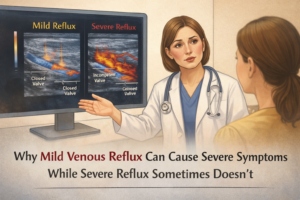
Yet observation across diverse patient experiences suggests something more nuanced. People described as having “venous reflux” can present with very different symptoms, clinical courses, and responses over time. Some experience meaningful improvement after targeted interventions, while others see little change. This recurring pattern highlights a central issue: a physiological finding is being treated as though it were a complete disease explanation.
Why this confusion persists
Several forces contribute to this framing.
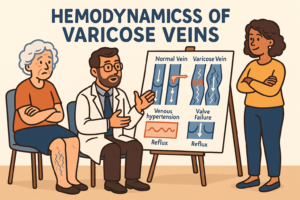
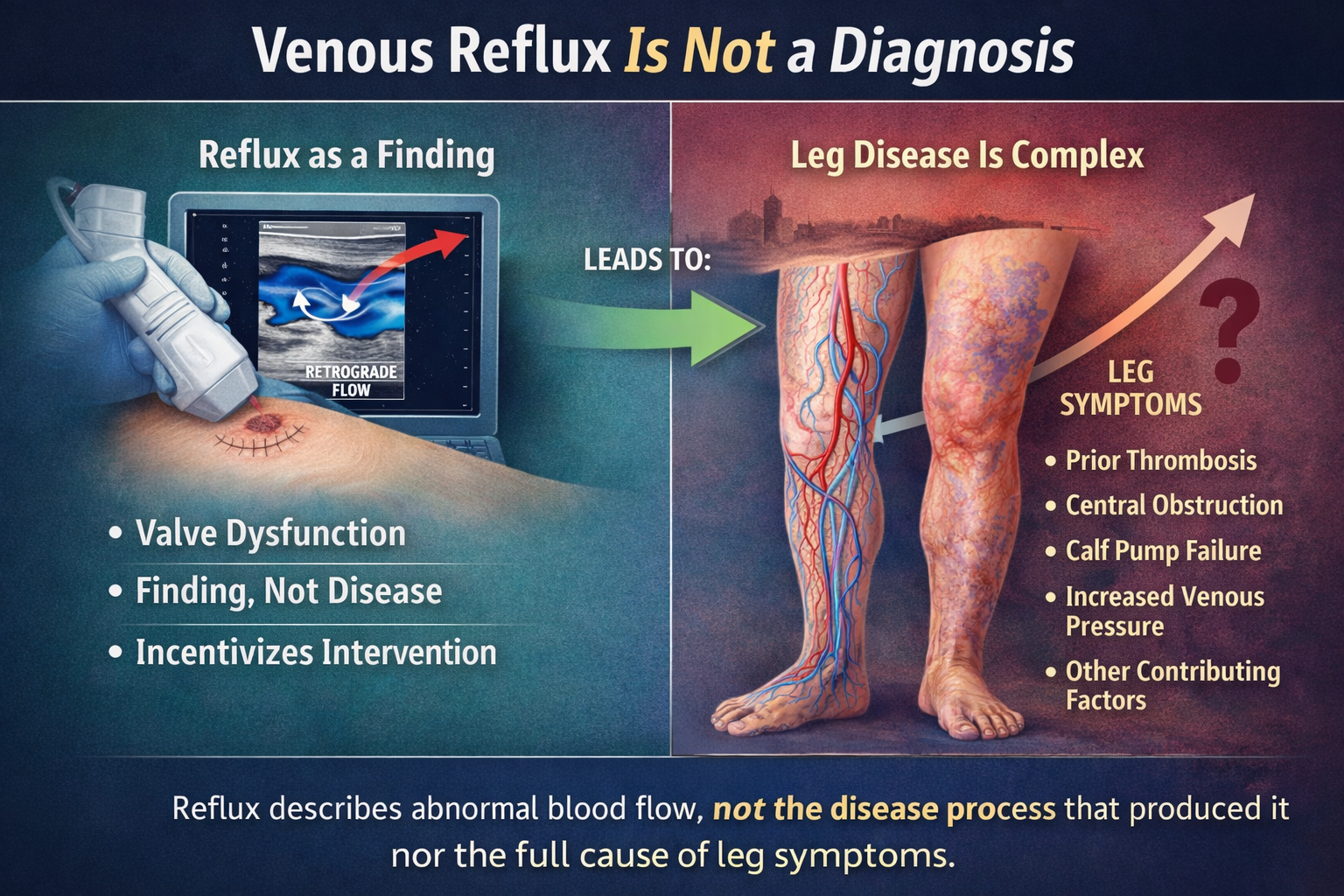
First, reflux is measurable. Duplex ultrasound provides clear, visual evidence of abnormal flow or valve behavior. By contrast, many contributors to leg symptoms—such as connective tissue changes, venous wall remodeling, inflammatory processes, calf muscle pump efficiency, prior thrombotic injury, or central venous influences—are less immediately visible and more difficult to quantify.
Second, language compresses description into meaning. The term “reflux” can sound explanatory, even though it simply describes what is happening in a vein segment. It does not, by itself, explain why it is happening or how much it contributes to an individual’s symptoms.
Third, care pathways often organize around identifiable findings. Once reflux is detected, it can become the dominant reference point, sometimes overshadowing broader context such as symptom pattern, distribution, progression, or coexisting conditions.
Finally, people naturally seek clarity. Being given a label can feel like receiving an answer, even when that label functions more like a test result than a full diagnosis.
The cost of narrow framing
When venous reflux is treated as a diagnosis rather than a finding, several consequences can follow.
Symptoms may be oversimplified: Leg discomfort, swelling, skin changes, or fatigue may be attributed primarily to reflux even when other contributors play a significant role.
Care pathways may narrow too early: Attention may center on a single mechanism while alternative explanations remain unexplored.
Expectations may misalign with outcomes: When an intervention addresses reflux but symptoms persist, frustration can arise—not necessarily because something “failed,” but because the initial framing was incomplete.
Opportunities for broader insight may be delayed: Chronic venous conditions are heterogeneous, and focusing on reflux alone can postpone a fuller understanding of disease pattern or progression.
In this sense, delay is not just about time. It is about how the problem is defined from the start.
Stating uncertainty openly
Several uncertainties are important to acknowledge.
Similar reflux patterns can be associated with very different symptom profiles.
The relationship between reflux correction and long-term change varies across individuals and contexts.
Imaging captures flow dynamics, but not the full biological condition of the vein wall, surrounding tissues, or systemic influences.
There is no universal threshold at which reflux has the same significance for every person.
Recognizing these uncertainties does not diminish the value of identifying reflux. It simply places it in appropriate context.
A more expansive perspective
When venous reflux is viewed as one piece of information rather than a standalone diagnosis, something useful happens. The conversation broadens.
A more comprehensive assessment can reveal contributors that were not initially considered—such as lymphatic factors, musculoskeletal influences, prior injury, systemic conditions, or lifestyle-related stressors. In some cases, this wider view helps direct attention toward forms of care, monitoring, or support that may not have been obvious when reflux was treated as the sole explanation.
This reframing does not reject reflux as irrelevant. It recognizes it as a signal—one that gains meaning only when interpreted alongside the full clinical picture.
The takeaway
Venous reflux describes abnormal flow. It does not, by itself, define a disease or fully explain symptoms. Understanding this distinction is not about withholding care or delaying action—it is about making space for better questions.
From an educational standpoint, progress comes not from narrowing focus, but from expanding context. When findings are interpreted within a broader assessment, pathways to care can emerge that might otherwise remain unseen.