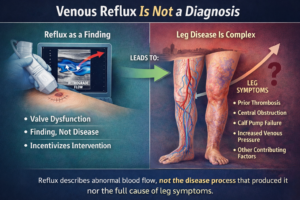


Chronic venous disease (CVD) is typically described in fragments. Reflux. Valve failure. Venous hypertension. Edema. Skin change. Ulceration. The language is anatomical and episodic, as though pathology emerges at a definable moment—a valve gives way, a vein dilates, a lesion appears.
Yet the clinical reality is slower and more continuous. Patients describe years of heaviness, swelling after work, dependent aching, transient ankle discoloration—symptoms that wax and wane, rarely urgent enough to trigger early investigation. By the time chronic venous insufficiency is formally diagnosed, the narrative often centers on structural incompetence: damaged valves, dilated superficial systems, perforator dysfunction.
What is frequently absent from this account is the concept of cumulative venous load—the aggregate mechanical and hydrostatic burden imposed on the venous system over time. Not a single insult, but decades of gravitational pressure, prolonged standing, obesity-related intra-abdominal pressure, pregnancy, occupational immobility, and aging connective tissue.
The disease is framed as anatomical failure. The variable that preceded it—the sustained load—quietly disappears.
Why it persists
The omission persists for structural reasons.
First, cumulative load is difficult to measure in clinical practice. Duplex ultrasound identifies reflux and obstruction; it does not quantify decades of orthostatic stress. CEAP classification describes severity, not history. The diagnostic framework privileges what is visible at the moment of examination, not what has accumulated invisibly over time.
Second, healthcare systems remain oriented toward discrete pathology. Interventions—compression therapy, endovenous ablation, sclerotherapy, surgery—target structural dysfunction. These are tangible, reimbursable, procedural responses to identifiable lesions. Cumulative load, by contrast, is diffuse, environmental, occupational, and metabolic. It resists procedural containment.
Third, medico-legal reasoning tends to focus on breach rather than burden. When ulcers develop or complications arise, analysis asks: Was reflux appropriately treated? Was compression prescribed? Was there delay in referral? These are legitimate questions within standards-of-care doctrine. Yet they presuppose that pathology begins at the point of visible deterioration. The slow accrual of hydrostatic stress—the foreseeable, progressive strain imposed on a dependent venous system—is rarely interrogated as part of the causal chain.
This is not scientific ignorance. The pathophysiology is well established. Sustained venous hypertension leads to endothelial dysfunction, leukocyte activation, microcirculatory impairment, capillary leakage, and inflammatory remodeling. Over time, these processes produce lipodermatosclerosis, hyperpigmentation, and ulceration. The cascade is cumulative by definition. But our explanatory models often compress it into late-stage manifestations.
Ethically, this narrowing of focus carries implications. When disease is described as late-stage structural failure, responsibility is implicitly individualized—genetics, weight, aging, lifestyle. The systemic contributors—occupational norms that require prolonged standing, inadequate workplace accommodation, delayed access to vascular assessment—fade into background conditions rather than foreground determinants.
The cost of delay
The cost of overlooking cumulative venous load is not abstract.
Clinically, it means patients are often treated reactively. Symptoms are normalized until skin changes become unmistakable. By then, microvascular damage is entrenched. Healing times lengthen. Recurrence rates rise. Venous leg ulcers—among the most costly chronic wounds in health systems globally—reflect not sudden catastrophe but prolonged pressure that was never conceptually centered.
From a risk-management perspective, the delay reshapes foreseeability. Venous ulceration is predictable in the presence of sustained venous hypertension. Recurrent episodes are common without durable control of hemodynamics. When early complaints are minimized as “just varicose veins” or “cosmetic,” the trajectory toward chronicity continues largely unchecked. The later question—why did this progress?—becomes harder to disentangle from the earlier failure to treat load as meaningful.
In tort analysis, causation in chronic disease is often diffuse, but not unknowable. If cumulative hydrostatic stress is a recognized contributor to progression, and if early indicators were present yet insufficiently addressed, then delay may intersect with breach. Not every adverse outcome reflects negligence; chronic disease evolves despite appropriate care. But the legal and ethical inquiry must at least acknowledge that progression was foreseeable, not incidental.
There is also a human cost less visible in documentation. Chronic venous disease restricts mobility, erodes sleep, impairs work capacity, and diminishes dignity through visible skin changes and chronic wounds. The psychological toll—social withdrawal, embarrassment, depressive symptoms—is documented but often secondary in clinical notes. Each of these consequences traces back, in part, to the slow, unmeasured accumulation of venous load.
When the variable is unnamed, its burden feels like fate.
It is important to state what remains uncertain.
We do not possess a precise metric for lifetime venous load. We cannot yet calculate a threshold at which hydrostatic stress irreversibly tips toward decompensation. Genetic predisposition, connective tissue integrity, inflammatory response, and hormonal influences all modulate individual vulnerability. Some patients with substantial reflux remain relatively asymptomatic; others progress despite modest anatomical findings. The heterogeneity is real.
Nor can every delayed diagnosis or ulcer be attributed to systemic oversight. Clinical practice operates within constraints of access, patient adherence, and competing priorities. Medicine cannot eliminate gravity.
The uncertainty, then, is not whether cumulative load contributes to chronic venous disease—that is physiologically coherent and empirically supported. The uncertainty lies in how prominently it should figure in our explanatory models, risk stratification, and standards of anticipatory care. At what point does ignoring the aggregate burden distort our understanding of duty? When does the failure to conceptualize load as central, rather than incidental, become a blind spot in both clinical reasoning and governance?
Chronic venous disease unfolds slowly, in dependent limbs subjected to unrelenting pressure. It is tempting to attribute its final stages to the moment valves fail visibly on ultrasound. But the more difficult truth is that the injury began long before that image was captured—accumulating silently, one hour of standing, one day of venous hypertension at a time.
Whether our frameworks—clinical, legal, ethical—are prepared to recognize cumulative venous load as the missing variable remains uncertain. What is certain is that the veins have been carrying it all along.